



Jeff was my roommate in medical school and later trained at one of the top orthopedic programs in the USA. He was a better student than I was. As kids, we climbed, weight lifted, and flew hang gliders together. We are now old dogs, so we compared injuries, and I have had more. Our dialog will amuse you. Here are a few other things we discussed:
Jeff says that stem cell injections work poorly for arthritis.
Steroid injections and cartilage removals create joint destruction and lead to the big surgery sooner. Both are a bad idea.
The operation time for joint replacements is usually short—between an hour and two hours.
Anticoagulation is used for months after some joint replacements.
Some people can use joints that seem worn out, according to the X-rays. Since these surgeries are done for symptoms, you do not need the procedure if you have little pain. Jeff said that if you have no joint space, most people get better with an implant.
Checking the urine and the teeth for infection before joint replacement is prudent because infections are life-altering and can spread from sources like these. Dental “spiral CT scans” can be used to be sure patients do not have hidden abscesses of the mouth.
I studied this subject when considering what to do with my sore shoulders, and I thought my listeners would like more information. Another factoid: RFK, Jr. told me that he had all six of his major joints--his hips, shoulders, and both knees--replaced or revised. All are working well.
The general principle is that you never consider these surgeries unless you have significant pain and are taking painkillers to sleep at night. If your discomfort is tolerable, you do not want to endure the risk, hassles, and recovery of a joint replacement or other surgery for orthopedic problems. Even if your X-rays look terrible, sensible surgeons do not recommend reconstructions or joint replacements when symptoms are modest. Many situations will improve if you are patient and carefully rehabilitate yourself.
You can investigate your case by getting x-rays and seeing the orthopedist if you have chronic, moderate pain. Find out who has the most experience with the procedure you might need and see what they think.
The hip replacement procedure won an award as the safest and most effective surgery of the 20th century. This is not entirely true; cataract surgery is better. Hip replacements rarely have complications, but if they get infected, it is life-altering. On the other hand, cataract surgery has almost no problems in experienced hands and consistently improves vision. Some newer lenses can help you see near and far, like bifocals.
Although knees are done more commonly, shoulder replacements are the second most predictable total joint surgeries after hips. In experienced hands, however, shoulders have excellent results with proper rehabilitation. If your tissues and body are reasonably healthy before the surgery, your chances of a perfect outcome are high. I had little pain and took no opioid painkillers after mine.
My friends have all had great results and needed no pain drugs after their knee replacement recoveries. However, published reviews of this surgery show that up to 50% of patients still require painkillers following the surgery. These also get infected more often than hips or shoulders. The factors that predict excellent results are good health, bone quality, and the surgeon's skill. Skill is directly related to the number of cases done—experience. Always ask your surgeon how many like yours he has performed.
Here is information about bone health and hormonal issues from Hormone Secrets:
I have osteoporosis. Can hormones help me? This is a significant health issue for elders—twenty percent of those over 65 breaks a hip. Many become nursing home residents; depending on the study, up to 58 percent are dead within a year. This dwarfs breast cancer as a public health problem. Although hip fractures occur mainly in women, they can also happen in men.
Hattie is 64 years old and works as a federal prosecutor. She is small, single, Chinese, and stressed. Her physician diagnosed her with “osteopenia” a decade ago. She treated Hattie in the office to a regimen of bisphosphonate injections and has followed her with dual-energy X-ray absorptiometry (DEXA) scans. But Hattie’s scan scores have gotten worse. When she had a hip replaced, the orthopedic surgeon told her that the bone was “crumbly.” Two years ago, Hattie began estrogen, selenium, DHEA, progesterone, vitamin K, testosterone pellets, and 10,000 IU of vitamin D. She recently started ipriflavone. Since beginning hormones, she can do jury trials and other high-intensity legal work like an attorney half her age. She was able to cut her Prozac dose in half. Her repeat DEXA showed that her bone density increased by 7 percent in two years. She is starting HGH and hopes to improve even more.
Physicians working with osteoporosis try first to eliminate causes such as steroids, smoking, and other drugs. After this, the pricey, FDA-approved bisphosphonate medications are usually tried. The industry promotes them for the prevention of bone thinning, but they are worse than nothing. They cause fractures, rotting jawbones, and even esophageal cancer. TheNNT.com summarizes the data, quoting a Cochrane meta-analysis. They say the drugs are ineffective for women without prior fractures and that they prevent bone breakage solely in the small group of women who have both osteoporosis on a scan plus a previously broken bone.
These facts make it hard to fathom why there are 80 million people using these drugs in the US. There is at least one good reason, however: our good doctors get about a 20 percent commission for dispensing medications like these in their offices. This is a terrific conflict of interest and would be criminal fee-splitting if physicians made a deal like this with another doctor instead of with a corporation. Another similar case is Lupron, the chemical castration agent used for prostate cancer. You and your insurance company pay $10,000 for each shot, and the doctors get their cut of the loot. See the oncology section of Butchered by “Healthcare” for more.
Although the original studies claimed these drugs decrease bone breakage, this medication class increases fractures of the largest bone in the body, the femur. They also produce cases of irreversible jawbone rotting. Plaintiffs have filed thousands of lawsuits against Merck alleging their bisphosphonate, Fosamax, caused these disasters. The company paid $28 million to settle twelve hundred of them. These drugs also increase the risk of atrial fibrillation.
Most people hate this medication class because the drugs make them feel terrible. One website lists over 40 side effects. In contrast, hormone treatment makes most people feel wonderful along with preventing and reversing osteoporosis. DHEA, testosterone, vitamin D, and estrogen all have positive effects. HGH alone can improve bone density by eight percent a year.
Here are some non-hormonal treatments that are safe but more speculative. Selenium may help at a dose of one gram a day, increased after a month to two grams a day. Vitamin K2, one milligram per day, might also be valuable. Ipriflavone, 600 mg per day, is an approved prescription treatment for osteoporosis in Japan that is over-the-counter in the US. It may help if you already have the condition.
I had progressive pain for five years in my left more than my right shoulder. I took painkillers almost every night for years to sleep. I had some fantasies about stem cell injections, but after a friend had successful shoulder replacements, I decided to get a consultation. Fortunately, I found a surgeon who had done more than 1000 and had been trained by the top shoulder replacement surgeons in town (Dan Acevedo, MD, at Kaiser Panorama City). So I decided to proceed.
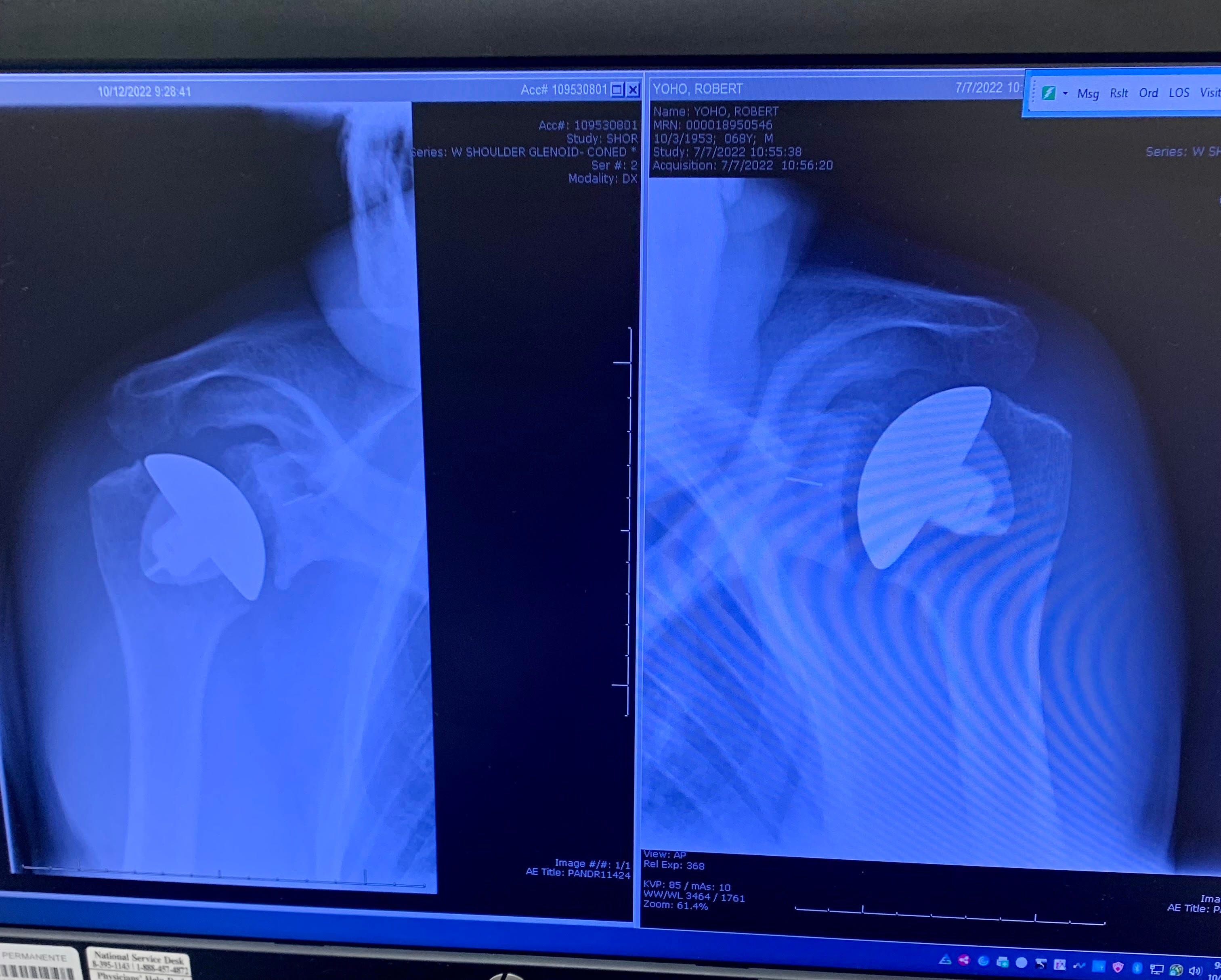
See my X-rays above. In recent years, orthopedists learned that long stems on the steel caps caused problems, so these were eliminated. The socket (glenoid fossa) is made of plastic and cemented in place with the same special glue used for the humeral head implant.
My surgeries were performed 4 1/2 months apart. Other surgeons recommend waiting six months to a year to allow complete recovery from the first shoulder. About 12 weeks following a shoulder replacement, the surrounding tissues become durable and can tolerate range of motion and strengthening exercises. Before that, only moderate stretching is recommended. I was nearly pain-free two weeks after each surgery.
These artificial shoulders last 15 to 30 years, about my expected lifespan. Replacing them is a hassle, but it can be done if they wear out for some reason. I plan to swim, lift weights, and do a little rock climbing. Wish me luck—at 69, I need it.
About the comments: I know that I am an acquired taste. The friends I cherish are the ones who tell me when I am wrong so I can sharpen my messages against their intellects. The rule here is that you can be as pushy as you want, but if I suspect you are insincere, I will kick you off (this has never happened to date). It is free speech--sharp sticks are tolerated. As I was writing Butchered by "Healthcare," I had a wonderful critic (thanks, M!) who treated me like a retarded stepson. She always got the message across, and I was never offended after I got used to her.









Share this post