



For new readers: HERE are links to download my CV, ebooks, the best recent posts, and instructions on searching my archives. Also, HERE are links to purchase OSR, DMSO, and chlorine dioxide products, where to find them, and more. Please review Judas Dentistry; the direct link is HERE. I need your help because a passel of mercury-intoxicated dentists are giving me one-star reviews. Finally, if you have a good story or are an expert who wants to be interviewed, please contact me at RobertYohoAuthor@gmail.com.
HERE is the Rumble link. This post is just a fraction of the interview content from above, so consider listening to it after you scan this post. It is one of my best.
Marsland is a nurse practitioner who works with Pierre Kory and Paul Marik. They are the geniuses who founded the FLCCC (Front Line COVID-19 Critical Care Alliance). This reflects well on Scott.
Scott was severely vaccine-injured by two Pfizer shots, went into heart failure, and all four of his heart valves started leaking. His ejection fraction went down to 40 percent. This is the fraction of blood expelled from the heart with each beat, and normal is 50-70 percent. He says he would be dead if he had not limited the damage with ivermectin, so he left his secure job to avoid another kill shot.
Scott describes learning about vaccine injury almost at the same time Dr. Kory did. They independently discovered how profoundly effective ivermectin was—COVID cures occurred sometimes in as short as two hours.
Kory had earlier completed a study on intravenous vitamin C treatment for COVID that lowered the death rate of sick patients by more than half. His hospital fired him. Marsland had an opportunity to work with Kory, recognized his integrity, and jumped at it.
Scott explains the spike protein and testing for it:
The spike protein targets the hippocampal area of the brain and turns off memory, joi de vivre, motivation, and other high-level functions. It causes micro-clotting, and we have a laboratory test for that.
Dr. Jordan Vaughn, based in Birmingham, Alabama, is the foremost United States expert on microclotting. He says the difference between microclotting and normal clotting is that normal clots have enzymes that break them down after serving their purpose. Microclots have amyloid, a very persistent denatured protein, and they are missing most of the enzymes required to break down clots.
We send blood samples to his lab in Alabama, and Jordan uses a stain to look at them under an electron microscope. He grades the microclots from 0 to 4. If someone has had several boosters, they typically have a 3, 3.5, or 4. Micro-clotting existed before the pandemic. People with a chronic disease were positive; we know that from banked blood. But now, we see very high levels because of the spike protein, which provokes this, especially in the vaccinated. Ivermectin blocks the impact of spike on red blood cells, platelets, and the endothelial cells that line blood vessels.
None of this was significant before the vaccine. COVID is not the primary problem, although it accelerates the clinical syndrome caused by the vaccine. At the beginning of the pandemic, if people got sick with COVID and then developed post-acute sequelae of COVID, they were at the very beginning of it. We didn't know that long-COVID was a thing yet. Thirty percent of our patients never got the shots, but some of them still act like they're vaccine-injured. The disease is a spectrum.
The spike protein is a pathogen, whether it's from having acute COVID or whether it's from the shots. It is one of the most toxic proteins ever introduced into humans. The list of diseases provoked by it is longer than my arm. We also use LabCorp’s spike antibody IgG test and a nucleocapsid and spike antibody, but the nucleocapsid only says that you have had acute COVID recently.
About 10% of our vaccinated patients have a spike antibody level that is off the charts—greater than 25,000 on their scale. These people are typically still working in places where they are around people who are getting boosted. Examples include nurses, doctors, physical therapists, teachers, and retail workers.
This is part of how we came to understand shedding. I had three unvaccinated patients with spike antibody levels of less than a thousand. In October 2023, a new booster came out. Each of them went into the hospital for same-day surgery. When we rechecked their spike antibody level a month later, all were higher than 25,000.
I used to go to the gym but stopped. I also used to go to Quaker meetings, but I would start getting a headache five minutes into the service. Then I figured out that all of my beloved Quakers were boosted, every single one of them.
For about two years, we've been using the spike antibody test as a proxy, an imperfect measure of spike burden. Until there is a test to measure spike directly, we use this test. It is like using a mirror to look for the vampire behind you. When we initiate therapies that break down spike, the antibody level generally decreases.
The subpopulation with long-haul and vaccine injury generally requires a low and slow approach, regardless of the therapeutic intervention. Many of them also have reactivated viruses, latent Lyme, mold toxicity issues, and so on.
People still actively engaging with the public have a high spike burden. This holds especially if they were vaccinated and more so if they got one or more boosters. We have to be especially cautious with them when initiating a treatment that will break down the spike because their micro-clotting can worsen and instigate a horrific reaction that will persist. They can lose trust.
Shedding from exposure to boosted individuals has contaminated the environment and perpetuated spread of the disease.
Marsland’s therapies
Ivermectin. Because of his personal experience, Scott recommends taking this continuously. If patients have doubts, he tries to get them to take doses as low as 3 mg daily. He believes .2 to .3 mg/kg/day is optimal (about 15 to 20 mg daily for a 70 kg person). Scott says that all of us—even the unvaccinated—now have abnormal blood clotting due to the shedding of spike protein from person to person. He says, “We've tested amyloid fibrin micro-clotting in thousands of patients, and every single person we've tested had some micro-clotting.”
Low-dose naltrexone (LDN) is the second most common therapy Scott uses. LDN can be dosed anywhere from 0.01-4.5 mg daily. Patients take 4.5 mg only after working up to it, but Scott said, “I have treated people with doses as low as .01 milligrams daily and seen clinical benefit.”
Almost everyone in the practice is encouraged to use a $550 PEMF machine (see below). This reduces inflammation, restores mitochondrial function, and decreases fatigue. Scott told me, “We have used it for more than 300 patients. We had an 87-year-old patient who had thoracic vertebral fractures and was scheduled for fusion surgery two weeks after our first visit. He got the device, and three days later, he canceled his surgery. The pain he'd had for 20 years completely resolved in three days. He just has to wear the thing for three hours daily.”
Sulodexide (SDX) is an anti-coagulant medication developed in Europe in 1972. It is safer than aspirin and more effective than Eliquis and Plavix combined. It is anti-thrombotic, anti-fibrotic, and inhibits platelet aggregation. It heals the lining of blood vessels, and it is anti-atherosclerotic. The trade name is Vessel. It is available inexpensively on the internet in bottles of 500 capsules. Although it is not approved for use in the United States, it has been approved for use and used since 1972 in many European countries. Our patients get it online at a Russian website. It comes in 250LSU (25mg) gelcaps, #50 in Italian boxes for 37.5€, or #60 from the Russian source. Scott writes about it in his Substack HERE:
In early June 2024 I wrote about the anticoagulant drug Sulodexide (SDX) in my Substack From Russia with love. The reference to Russia is because most of our patients have sourced it online from a Russian platform, but all SDX is manufactured in Italy. The packaging and the little red gel tabs are the same, and the dosing is 250LSU, which is 25mg. The only differences are the language on the box and the number of doses included. The Russian version has sixty gel tabs, and the Italian version has fifty.

Russian on top, Italian below In the last two months, several patients of the Leading Edge Clinic have been implementing this therapy in earnest, and we are seeing a wide range of benefits with most. A few patients haven’t tolerated it, meaning that their symptoms got worse, and some used it for a month without noticeable benefit, but most are reporting positive results early.
How do I love you, Sulodexide? Let me count the ways. SDX inhibits thrombin in a similar fashion as Eliquis and Xarelto, and it also inhibits platelet aggregation with other platelets, decreasing stickiness of the lining of blood vessels, like Plavix/Clopidogrel. But wait, there is more. It is anti-atherosclerotic for those in the crowd who have coronary artery disease. It is anti-fibrotic, breaking down the fibrotic changes we see in blood and tissue due to the spike protein. Perhaps most importantly, it repairs the glycocalyx, healing the endothelial cells that line the blood vessels in our body. Vessel, as manufacturer Alfa Sigma calls it, is a great name for the drug.
DMSO is a profoundly effective amyloid-dissolving agent that works well with
Sulodexide. You can work up to one and a half teaspoons orally twice daily. Learn more and buy it at the sources in the top paragraph of this post.
Hydroxychloroquine
Alinia (nitazoxanide) 500-600mg twice daily for five days. Scott stops it sooner if the symptoms go away or if there are GI side effects. This antiparasite drug is conventionally used for giardia.
Fasting is the most effective way to break down spike. Scott recommends 72 hours twice a month, and water is permitted. He says drinking bone broth while fasting makes it more tolerable, and fats such as olive, coconut oil, and butter can be consumed without breaking the fasting ketosis. He told me, “One of my patients used to have a spike antibody level above 25,000 after two mRNA vaccines. He has been religious about doing 72-hour fasts twice a month, and we watched him come down out of the clouds to 18,000 to 10,000, and finally to under 4,000 over about a year.” (THIS cancer video is excellent and has information about fasting. Thanks, Kat!).
NAC (N-acetyl cysteine) is essential for making the powerful antioxidant glutathione. 200 mg (from Vitahealth Apothecary in NYC) should be taken twice a day at the start. Scott said:
NAC completely changed the clinical landscape in our practice. We could see the difference in the labs—the spike antibody dropped. In one patient, I saw it drop 5,000 points in the month after starting NAC. This isn't NAC from Pure Encapsulations or another supplement provider; it comes from ZeroSpike.com, a renegade nonprofit with only ten people in Italy. The way they augment the NAC is proprietary, but it breaks the disulfide bond between spike and ACE2 receptors. 99.8% of the spike that impacts it denatures and breaks down into almost 100 pieces that the body can then metabolize and eliminate in the urine.
Dr. Kory, another partner, and I will soon be distributors for a ZeroSpike urine test that measures spike breakdown products using mass spectrometry analysis. The test will be affordable.
Lithium orotate is a trace mineral that is anti-inflammatory for the nervous system. It costs pennies and can be obtained from Horbaach Co. The first dose should be tiny, and according to Dr. Michael Nehls, 5 mg a day is optimal. It is inexpensive and safe. Scott says:

I prefer Horbaach ($15 for 130mg of Li Orotate, which equals 5mg of active Li) or Pure Encapsulations 1mg or 5mg from FullScript.
The dose is 130 milligrams of lithium orotate and five milligrams of active lithium. It costs $15, including shipping for half a year's worth. Lithium keeps neurons from dying, reestablishes connections between neurons that have lost each other, and helps restore the hippocampus's function in part by globally decreasing neuroinflammation. I have measured neurotransmitters on more than 100 patients and seen them come back into balance. We use the ZRT urine neurotransmitter test, which lists 27 neurotransmitters from GABA to glutamate to catecholamines. In vaccine patients, 14 to 16 of these are abnormal. When they use lithium, these return towards normal.
Life Extension’s product provides 1mg of lithium and presumably contains 23 mg of lithium orotate. Take one of those a day to get a 1mg daily dose or, for treating a known case of brain inflammation, five for a 5 mg daily dose.
Pure Encapsulations makes five mg and one mg lithium supplements. The 1mg product is HERE.
Kory and Marsland started investigating chlorine dioxide after I arranged two staff meetings with their clinical group. They are first considering commercial products such as Snoot Spray. Although the manufacturer cannot advertise medical benefits, even very low doses of chlorine dioxide have systemic effects and are profoundly beneficial. See the first paragraph of this post for information on how to obtain them and more.
Cautions
Scott has observed visual disturbances with ivermectin in patients taking as little as .6 mg/kg/day.
He says that the people at Vitahealth Apothecary have seen patients who use fenbendazole and who had excellent results when they first took it. But when they stop it, if the cancer comes back, it may be chemo-resistant and aggressive. He also notes that the drug is not approved for humans.
Marsland told me that he sometimes feels like he is in a zombie movie where people are dying all around him. I asked him whether it was really that bad. He replied:
Unfortunately, it is. I think that the new administration can't come into office soon enough. We need to accelerate the creation of a truth and reconciliation committee. The entire population needs to understand the bioweapon that has been foisted upon us, both in the pandemic and in the shots. And I don't know about you, Robert, but knowing what I know, I always hear more stories just moving in the world. A growing number of people are saying, hey, this 30-year-old just died of brain cancer. This 20-year-old just developed seizures and can't work anymore. That's not normal. The ones that have had four vaccines or more are dropping dead.
Influences
Robert O. Becker, an orthopedist and the author of The Body Electric, a book with over 1200 reviews averaging 4.2 stars. He is the rarest of academic animals: a researcher, teacher, and clinician. His research is the basis of the Arc Microtech device and the origins of modern PEMF devices.
Tina Peers, an MD in London, treats patients like Scott’s. She told his group about ARC Microtech, a $550 PEMF (Pulsed Electromagnetic Field) machine. Invented by Ian Thirkell, a retired London police investigator, it was developed for horses. However, when the jockeys were exposed to it, they realized its value and started using it on themselves. The highly respected PEMF BEMER (Bio-Electro-Magnetic-Energy-Regulation) is more than ten times as expensive.
Cost and scheduling
The cost to see Scott or Dr. Kory is the same: $2,350. Scott says,
Pierre and I have, in our mutual estimation, a comparable level of expertise in treating long-haul. The charge is for an hour of intake and two half-hour follow-ups over the next three months. Ongoing nursing support is included.
People are used to paying small co-pays for terrible healthcare, so it seems like a crazy amount of money, but we never have medical assistants see you. We have RNs.
All appointments are virtual. You can reach their Leading Edge Clinic HERE or at LeadingEdgeClinic.com. Dr. Kory and Scott are licensed in several states and have Indian reservation medical licenses, which would protect their ability to practice if the Cabal manages to revoke their licenses.
Quirky Yoho ideas
Despite all the horrifying information about shedding and the ubiquitous laboratory-proven shedding and spike illness he has seen, Scott is so optimistic about the treatments that he says he is “working his way out of a job.” I reassured him that that would never happen and that plenty of new patients needed his help.
He emphasizes that combination therapy works best. My question is, when is enough enough? How much medication can we tolerate? How much complexity can we handle? Of all the above ideas, the elephants in the room are chlorine dioxide, DMSO, and fasting, which cost almost nothing. Scott adds that SDX has a substantial clinical effect. Taking ivermectin chronically is also a good practice, especially for people who are exposed to the public. It has many positive effects, even on Parkinson’s.
Since this is new information for me, I need to consider the rest of Scott’s recommendations before using them. But if you are sick—and certainly if you fear for your life—you had better throw out all your hand grenades at once.
I could not resist spending $460 on the equine PEMF machine (it was a Black Friday special!). I had been casually considering a BEMER, but that costs over $6000, and I feared I would have buyer’s remorse. While practicing, I bought a lot of electronic junk that just took up closet space. I still have some that I cannot stand to toss.
Marsland sees a parade of sick people who desperately need help. As I think about him, his patients, and his vax injury, I once again consider the specialist syndrome. They see the world through the lens of their narrow experience. But as always, things are neither as bad nor as good as anyone believes.
I dutifully take handfuls of supplements, but what I feel the most are hormones—melatonin, DHEA, and testosterone. These, plus estrogen and progesterone, work miracles for women, too. Chlorine dioxide makes me tired. I always feel best when I skip it all for a few days.
At the end of the interview, I said:
Is there anything else you want to say, Scott?
Marsland: This has been fun. I write a Substack at lightningbug.substack.com. It's a personal reflection, and I blend that with actionable clinical information.
Yoho: I subscribed. If we are done, I can't resist this. Beam me up, Scotty. Sorry, I know you've heard that nonsense before.
Marsland: I love hearing from you and hearing you call me Scotty.
Disclaimer: Scotty has no financial interest in any company mentioned here. Neither of us is dispensing medical advice in this post. Use your best judgment and get honest help from a provider if you can find it.
An excellent reference is HERE.
Errata: 1. Sorry, I misspoke. Snoot is not FDA-approved. It is considered a cosmetic, and the manufacturer makes no medical claims. 2. Scott said the DMSO dose was 1.5 tablespoons twice a day in the podcast. He meant to say teaspoons.
Parting shot #1: how to use a $20 digital scale
You should consider powdered supplements. They are economical and far purer than capsules or tablets, which contain fillers and, God only knows what else.
Find the button and zero your scale first with the empty scooper on it. Do not make a mess by putting powder on your scale, as I did.
The images below are 1/8 teaspoon. The top one is the melatonin I got from BulkSupplements.com, and the bottom one is OSR, which is heavier. That melatonin dose of 276 mg is OK for me, and you can go lower for OSR if you want. I obtained powder DHEA, magnesium glycinate, and pregnenolone and am trying to find ivermectin. I mix these in a bit of honey before eating them at bedtime.
Parting shot #2:
Katrina Lewis revised her cancer post HERE. She says that fenbendazole has been reported to cause cancer recurrence if stopped, and her doctors no longer recommend it.
She also says 10,000 units of vitamin A daily prevent ivermectin-related ocular problems such as seeing flashing lights. Monthly eye exams are recommended, but I wonder if you need them if you take the A only five days a week.
The standard ivermectin dose for cancer is 1.5 to 1.7 milligrams per kilogram per day in one dose. You can obtain it from the Indian pharmacies listed in the links in the paragraph at the top of all my posts or American compounders with a prescription. Since I weigh 70 kilograms, if I had cancer, I might take 105 milligrams or a bit more daily indefinitely.
Ivermectin is cheap and super safe, but melatonin is cheaper and safer. Anyone over 45 should be using it.
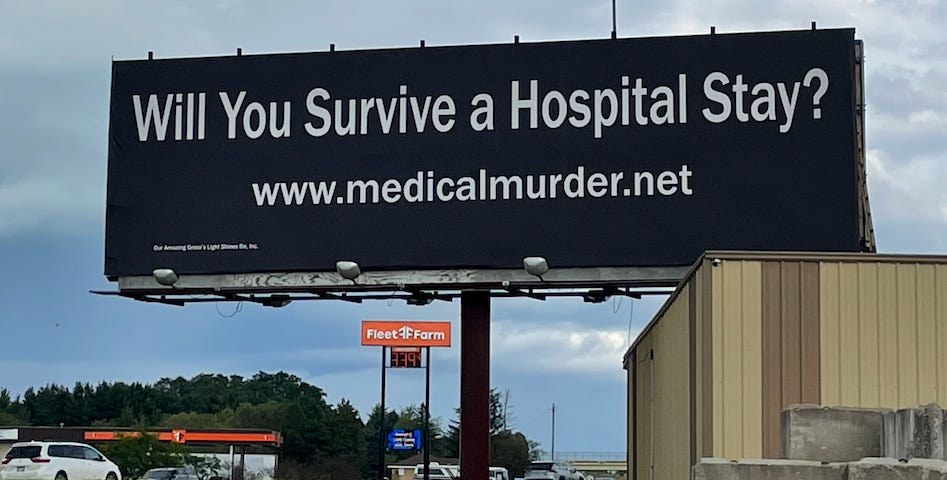
Parting shot #3:
This is one of Scott Shara’s sixty (60) billboards surrounding the hospital where doctors killed his daughter. He is suing them. Subscribe to his Substack.
#4: I need more editors
I would be helpless without them. I have some great ones, but I could use more. There are no required assignments, deadlines, or long-term commitments, and I learn from your perceptions, regardless of your level of sophistication.
Like anyone, I get infatuated by my writing and occasionally need to be brought up short. Some of what I send you will not be refined, and some may not be worthy of publication. I need blunt honesty and no inhibitions about telling me something sucks. Most of what I send requires only a quick scan. Reply directly to this email if you are interested.









Share this post