


For new readers: HERE are free links to my ebooks and best recent posts.
Age-related macular degeneration is a disease of a five-millimeters-wide area of the central retina where light is focused. The rest is unaffected. This macula is only 2 percent of the retina. It provides only a tiny fraction of the visual field, yet almost half of the brain’s visual cortex is used to process macular information.
The macula is responsible for central vision, sensing color, and perceiving fine details. AMD can create blurred vision or even blindness in the center of what is visible. When it progresses, driving, reading, and facial recognition are affected. Ten percent of people in the US over 50 have AMD, and in its late phases, vision is threatened.
Although I had been seeing a Kaiser retina specialist for several years, he only told me that I had a little “wrinkle or scar” on my retina. He obviously knew I had AMD, and must have thought that since there is no established therapy for my early stage, he did not need to tell me. But when a Costco optometrist told me the full truth, I began researching.
“Dry” macular degeneration is the initial phase, and my scans showed the characteristic separation or swelling in the area. The “wet” type happens later, as the disease progresses. The decline is sometimes rapid, and severe central visual impairment can result. Visual hallucinations and flashing lights may also occur (Jeez!).
Act #1: Ophthalmologists tell me that little can be done
There's no way to reverse damage from dry macular degeneration... [to] slow its progression, [Take] vitamin supplements, eat healthy, and do not smoke. (Mayo Clinic)
[The] exact cause is unknown, although genetic and environmental factors are thought to play a role. (HopkinsMedical.org)
Red light and other retinal treatments are useless and have never been studied with double-blind, placebo-controlled trials. (Kaiser opthalmologist who examined me)
No cure or treatment restores the vision already lost. (National Institutes of Health)
I knew there had to be more to the story. I also smelled a rat when I read that AMD is largely genetic. It sounded like the same Rockefeller medicine nonsense that I had been studying for Parkinson’s and other neurological diseases.
The entire eye industry sees the eye as a static camera lens rather than a dynamic biological system that gets better or worse depending on the stresses it is subjected to. Some of these, such as reading on computers for many hours, gradually damage the eyes. Others, such as sunlight exposure and spending time outside using the eyes to scan distances, improve eye function. These “hormetic” effects are analogous to the favorable effects of exercise.
Act # 2: Red light reverses macular degeneration and other eye diseases
I recently looked at the benefits of sunlight and wrote about red light treatments HERE. I suspected these would help, but was suspicious of red light experts because they all seemed to hawk products through affiliate programs. As Upton Sinclair wrote, “It is difficult to get a man to understand something when his salary depends on his not understanding it.”

Above: I am sitting with the SaunaSpace.com red lights ($1500) shining on my legs and other parts. After a few weeks of doing this three hours a day, my wife noticed that my shins were burned. Substack distracted me so much that I ignored what was happening. Since near infrared does not burn, it was the far infrared heat that caused the injury. Don’t say anything to me—my wife already did that two dozen times.
My next move into the red light “space” was when Dr. Zulia Frost, the medical director of Flexbeam, sold me one for $500. It is a skin-contact (or near-contact) device, she guaranteed results, and she was convincing.

Model not included.
Zulia suggested I put it on my ankles to help the arthritis. She said that if I used it on my belly, I could tell my aching gut microbiome to start working for me instead of against me. I tried it 45 minutes daily for a few weeks, but the bacteria, like my kids, DFL to me.
Since I noticed no improvement, I was about to give it to my chiro buddy. However, my interest spiked when Polymath Paul sent me Mark Sloan’s video about red light’s effects on vision.
Commentator Mark Sloan reports that red lights are safe and effective.
In the video below, Sloan cites the literature documenting the magic that near-infrared lights work on eyes. I watched it several times because it gave me hope. Mark says that in 50,000 studies of red light, no burns, side effects, or eye harm has occurred.

Sloan’s Medium article featuring this video is HERE and on his website HERE.
Red and near-infrared light protect against ultraviolet and burning. Since 95 percent of what tanning beds emit is UV, they would be safer if they had 50 percent visible, red, and near-infrared bulbs.
The sun and tanning beds help the body produce vitamin D but can burn. Red light does not have these effects.
Red light therapy is also called “noninvasive photobiomodulation.” Here are the results of a few studies:
Age-related macular degeneration improved. Patients averaged 63 years old. Four treatments of near IR laser treatment: 95-97 percent had improved vision lasting 36 months
Both young and old patients showed amblyopia improvement after near-IR laser treatment. 90 percent of eyes improved, and this lasted at least six months
A patient reported to Mark that her eyes improved to nearly 20:20 using a 24-watt red LED device.
A 2016 review of retinal diseases surveyed all the studies on low-level laser treatment of diabetic retinopathy. It was successful.
Methanol-related retinal damage responds to red light.
Mark says that eye damage is related to unsaturated fatty acids oxidizing and accumulating in the eyes. These are found in seed oils. Replacing them with animal fats, primarily from beef, sheep, coconut oil, and butter, and using red lights, can reverse this trend. In contrast, polyunsaturated fats (PUFAs) are inflammatory and damaging. See my recent episode about this HERE.
Rockefeller medicine sources claim, in contrast, that eating a diet high in saturated fat causes macular degeneration. Whom do you believe?
Dr. Zulia was concerned about safety
I asked her if my eyes would improve if I stared into her light’s uncanny redness. She wrote:
Yes, there is plenty of evidence for RLT's eye benefits. Some commentators think it is entirely safe because most devices that use RLT are cosmetic-grade, which is weak. However, in recent years, the industry has moved toward the ‘recovery’ market, and much stronger diodes are used. They are too powerful for eyes. Flexbeam is a leader in this field.
Flexbeam can cause damage if the eyes are directly exposed to it, particularly for people with macular degeneration.
I then asked Z if it was nevertheless reasonable to treat my eyes for a few seconds a day. She replied:
After consulting with our engineer, 3 - 4 minutes at 20 cm from the device in program two would be ok for you to do daily.
Eyes should be closed, but follow your intuition and stop if you feel it’s too much.
You need to take breaks; for example, if you use it for five days, take one or two days off, then start again.
You should experience improvements in 3 - 4 weeks.
I act like my kids and my gut bacteria—I DFL. Instead of taking Zulia’s advice, I started using the most powerful program (# 3) for 30 seconds, five days a week, two centimeters from the Flexbeam with my eyes open. I have also been putting DMSO on my eyelids. This penetrates into my eyes.
Before you try any of this, do your homework. If you must have a Flexbeam, use this LINK to buy one at a discount. The coupon code “robertyoho” will give you $60 off, and this LINK will make you an affiliate like me. I donate all profits, but you may keep yours.
Esther Joy van der Werf, a Bates method trainer, is unconcerned about the dangers of sungazing
She said looking at the sun for thirty seconds was safe because the sole eye injury ever documented was in a tied-up monkey. He was forced to look directly into the sun for long periods with his eyes pinned open. (A reader reminded me that eye damage, especially cornea burns, can occur at high altitudes, and I stand corrected about that.) Esther also recommended relaxation, walking in nature, and decreasing eyeglasses usage.
After the consultation, I started to view her work through Occam’s Razor. This is the principle that one or a few causes for something are more likely than many. I speculated that sun exposure or even red light alone might be the critical factor for visual improvement. Esther thinks I am seriously deluded.
Act #3: Jeffrey Luttrell, MD, prevents macular degeneration progression with a retinal laser
I ran across his website while looking at red-light ocular therapy and booked an appointment at his office in Beverly Hills. He also has one in Florida at The Villages, a massive senior housing complex that is the big brother of California’s Leisure World. (Off-topic snark: these places have the highest STD rates in the nation.)
Luttrell is a senior opthalmologist who uses a laser to create retinal “thermal effects” that decrease macular edema and prevent the progression of the dry to the wet type. He has thousands of successes that prove it works. Contrary to my other ophthalmologist's claim above, data like this requires no controlled trials.
The procedure takes only a few minutes and is risk- and pain-free, as far as I can tell. Luttrell recommends repeating it every three months indefinitely. He says many wavelengths might work.
Dr. Luttrell wrote a book about his experience, Modern Retinal Laser Therapy (2023) HERE, and is starting a chain of collaborators. His website is visionprotection.com, and his colleagues are jealous and critical.
I had the treatment once. When I got the bill, the $1800 seemed like a jab in the eye, but considering the alternative—an actual needle stuck in my eye every month—it was almost painless.
Act #4: What did I finally do?
As always, the lessons learned were more important than the exact outcome. I found once again that little in conventional medicine can be trusted. Just as my study of root canals saved my wife’s life, I would have to again use my wits and research abilities to survive.
By the time I got through Acts #2 and #3, I was sure my problem was solved. Recently, however, I discovered inexpensive methods that might cure rather than stall my macular degeneration. I looked at several:
Chlorine dioxide. Kalcker’s eye formula is HERE; this is 30 ppm, and others recommend no more than 20. Source’s story: My opthalmologist told me that I have a deterioration of my retina, causing a hole to appear. I started the [CDS oral] protocol from 5ml (in 500ml water) and later increased it to 10ml. I [also] made eyedrops with 1ml of CDS in 10ml water [far stronger than Kalcker recommends]… I used this morning, noon, and evening for a month. [Three months later], the optometrist showed me the pictures on the screen and said, "Congratulations, very few people were lucky enough to have their retina repaired itself like this."
DMSO alone. Source: 75 % / 25% water. Use two drops in each eye twice a day. I know six case reports of dry macular degeneration cured with this.
Combining #1 and #2 in a dropper bottle. From a Thai source: 20 ppm CDS and one drop DMSO is reversing his AMD.
Diluted injectable ivermectin as eye drops. Several sources: This cures some cataracts. The formula is 1/8 tsp salt, 2 tsp warm water, and 1/2 ml of 1% liquid injectable ivermectin. Some use veterinary. It can be stored n a dropper bottle purchased from an online health food store. One report: My mother’s cataracts disappeared within a month. She used two drops twice a day in each eye.
We know about ivermectin. When taken orally with 440 mg of fenbendazole, it halts many systemic cancers at doses of 100 to 150 mg a day. It is a harmless, Nobel Prize-winning drug with four billion doses given to humans. Why would it not cure macular degeneration?
Here is what I am doing now. In addition to my oral chlorine dioxide program, I sun gaze, use DMSO eyedrops, and look into my Flexbeam five days a week. I plan to have the Costco optometrist scan my retinas every three months to monitor my progress, and I will report back to you soon.
I am not ghosting my opthalmologist. He is a good dude, I trust him, and I have a film under one artificial lens that needs to be lasered off. But he will never learn my other plans unless you tell him.
Selected sources
Mark Sloan's website is EndAllDisease.com. I find his thinking interesting and have been hanging out there some recently. As I browsed his work, I began to respect his sophistication and comprehensive references. He says he has “Over 1,000 Hours of Free Video Content to Expand Your Knowledge and Consciousness.” He is not a clinician, however, and has never had to bear responsibility for his opinions in a healthcare setting.
By Mark Sloan:
Red Light Therapy: Miracle Medicine
Improving Eyesight with Red Light Therapy
Your Complete Guide to Red Light Therapy
The Ultimate Guide to Methylene Blue: Remarkable Hope for Depression, COVID, AIDS & other Viruses, Alzheimer’s, Autism, Cancer, Heart Disease Yoho comment: excellent. See also my MB post HERE.
Low-level laser therapy improves vision in patients with age-related macular degeneration (NIH, 2008)
Objective: The objective of this study of a case series was to examine the effects of low-level laser therapy (LLLT) in patients with age-related macular degeneration (AMD).
Background data: AMD affects a large proportion of the elderly population; current therapeutic options for AMD are limited, however.
Patients and methods: In total, 203 patients (90 men and 113 women; mean age 63.4 +/- 5.3 y) with beginning ("dry") or advanced ("wet") forms of AMD (n = 348 eyes) were included in the study. One hundred ninety-three patients (mean age 64.6 +/- 4.3 y; n = 328 eyes) with cataracts (n = 182 eyes) or without cataracts (n = 146 eyes) were treated using LLLT four times (twice per week). A semiconductor laser diode (780 nm, 7.5 mW, 292 Hz, continuous emission) was used for transconjunctival irradiation of the macula for 40 sec (0.3 J/cm2) resulting in a total dose of 1.2 J/cm2. Ten patients (n = 20 eyes) with AMD received mock treatment and served as controls. Visual acuity was measured at each visit. Data were analyzed retrospectively using a t-test.
Results: LLLT significantly improved visual acuity (p < 0.00001 versus baseline) in 162/182 (95%) of eyes with cataracts and 142/146 (97%) of eyes without cataracts. The prevalence of metamorphopsia, scotoma, and dyschromatopsia was reduced. In patients with wet AMD, edema and bleeding improved. The improved vision was maintained for 3-36 mo after treatment. Visual acuity in the control group remained unchanged. No adverse effects were observed in those undergoing therapy.
Conclusion: In patients with AMD, LLLT significantly improves visual acuity without adverse side effects and may thus help prevent vision loss.
Photobiomodulation for the treatment of retinal diseases: a review (2016)
Photobiomodulation (PBM), also known as low-level laser therapy, has recently risen to the attention of the ophthalmology community as a promising new approach to treat a variety of retinal conditions, including age-related macular degeneration, retinopathy of prematurity, diabetic retinopathy, Leber's hereditary optic neuropathy, amblyopia, methanol-induced retinal damage, and possibly others. This review evaluates the existing research about PBM applications in the retina, focusing on the mechanisms of action and clinical outcomes. All available literature until April 2015 was reviewed using PubMed and the following keywords: "photobiomodulation AND retina," low-level light therapy AND retina," low-level laser therapy AND retina," and "FR/NIR therapy AND retina." In addition, the relevant references listed within the papers identified through PubMed were incorporated. The literature supports the conclusion that the low-cost and non-invasive nature of PBM, coupled with the first promising clinical reports and the numerous preclinical studies in animal models, make PBM well-poised to become an essential player in treating a wide range of retinal disorders. Nevertheless, large-scale clinical trials will be necessary to establish the PBM therapeutic ranges for the various retinal diseases, as well as to gain a deeper understanding of its mechanisms of action.
Mark Sloan’s anecdote from his EndAllDisease.com. His reader Kayla reported a dramatic improvement in her myopia using a handheld red light therapy device.
It is an astounding 3200x more potent than the laser device used in both studies above. Using our red light therapy dose guide, I calculated the exact treatment time and distance required using our handheld device to get a similar dose to what was administered in the two studies. To get a 1 J/cm2 dose using the 24-watt handheld device, apply the light for 5 seconds from a distance of 5cm or 50 seconds from a distance of 50cm. Of course, given red light’s astounding safety profile, never be afraid to experiment with more. Five minutes, 10 minutes, 20 minutes, 30 minutes, or more are all good treatment times to experiment with.
“Legal” disclaimer
I do not practice medicine, and I am not endorsing any of this for your use. I have not reviewed the supporting material completely. That said, I find it credible and will continue to study it as long as I can see. You should, too.
Parting shot:
Flexbeam also recommends its product for pets, but when I treated our 150-pound Cane Corso to a session, he refused treatment by jumping away and barking deeply. I pick my battles with him—his bite strength is 700 pounds per square inch (PSI), which is stronger than a lion’s. For reference, pit bulls can only bite about 300 PSI.

From the Flexbeam website HERE.
Appendix: wavelength basics
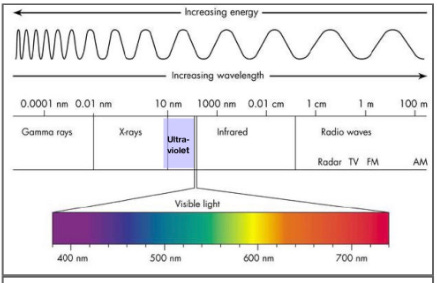
Of the whole solar radiation spectrum, we are concerned with:
ultraviolet (purple rectangle to the left of visible)
visible in the middle (the sliver that is blown up as the color chart)
near and far infrared (box on the right).
Sixty percent of sunlight is near-infrared (the left half of the box that is marked infrared), 43 percent is visible, and only 5 percent is ultraviolet. This helps the skin make vitamin D but can cause burns.
You need to be a paid subscriber to read further, ha.









Share this post