


This takes 22 minutes to listen at normal speed and half that to read it. It took me over 12 hours to find, edit, and compile this information.
I. SADS is a fraudulent diagnosis
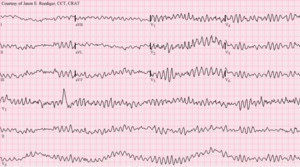
IN ITS SADS ARTICLE, WIKIPEDIA kindly shows us what your EKG would look like if this syndrome caused ventricular fibrillation and killed you:
Wiki censors negative information about the clot shot, so they do not mention it in their article:
Sudden adult death syndrome (SADS), sudden unexplained death syndrome (SUDS), and sudden unexpected nocturnal death syndrome (SUNDS), are sudden, unexpected deaths of adolescents and adults, mainly during sleep… [This] can be caused by medication, myocarditis, cardiac conduction disease, genetic connective tissue disorders, or other causes.
The following is abridged from Chaval’s post.
Countless adults 40 years and younger are dropping dead, and authorities are calling this Sudden Adult Death Syndrome. This is a new, supposedly mysterious disease, and it has been recognized by insurance companies, independent media, and some physicians.
Left unsaid, but playing out in the data, is that these young people are passing away in the prime of their lives after having been vaccinated with one or more Covid inoculations. There has not been a single case report of an unvaccinated person in this age group suddenly dropping dead without another cause.
Over the past two years, doctors, immunologists, and virologists around the globe have been warning about the Covid vaccine. They predicted myocarditis and a host of other diseases. They also foretold “antibody deficiency enhancement,” which is a decline in immunity to Covid infection after the “vaccination.”
These mRNA injections have been proven to stimulate prolonged manufacture of spike protein in the host’s body. This produces many ill effects including clots in the blood, heart, brain, and other organs. How long this continues is unknown, but what is clear is that the more times a patient is “boosted,” the greater the risk.
SADS resembles SIDS (Sudden Infant Death Syndrome). This similar name was coined decades ago to put a label on the epidemic of infants dying suddenly without a recognized cause.
With this background, the old mystery of what causes SIDS becomes transparent. It was a hoax created to explain away injuries caused by other vaccines. A new study of SIDS since the 1990s based on the Vaccine Adverse Response System (VAERS) found that nearly every baby dying from SIDS received a childhood vaccination within 1-7 days before passing away. The SIDS label had fooled us so thoroughly and for so long that someone hatched the SADS swindle to dupe us again. And, just like they did for SIDS, the legacy media and medical journals are now trying to normalize SADS.
As of this writing, there have been 28,532 post-vaccination deaths reported in VAERS and over 1.287 million adverse reactions. A Harvard study showed that the true figures could be as high as 10 to 40 times that. Many nurses are also saying that they were ordered not to report these events. And according to CDC whistleblowers, the agency has removed as many as 12,500 records of the most serious cases from the database. Finally, the media is failing to report that the vaccine injury compensation programs are overwhelmed.
Most of us know a healthy person who died suddenly without warning. We have also heard about celebrities and professional athletes dropping dead. Single car “vaccidents” have been on the rise, and previously healthy pilots have mysteriously suffered career-ending ailments. Several have died hush-hush in midflight.
A Pharma executive, Jose Maria Fernandez Sousa-Faro, recently paid to be injected with saline to get a vaccine passport. Industry insiders say that many athletes and celebrities have done this as well. The elitists’ hypocrisy is plain to see and tells you all you need to know about vaccine safety.
Unless you have intentionally chosen to ignore the obvious evidence for two years, you understand that the clot shots do not prevent the spread of Covid, do not prevent infection, and are not vaccines in the traditional sense; rather, they permanently alter genes. The jab has profound risks and no net benefit.
What we are seeing now has been variously described as Stockholm Syndrome, mass formation psychosis, or cognitive dissonance. Although some people are willfully ignorant, the legacy media and the medical community are potent propaganda machines that have hypnotized a full third of us. Other people are falling into line to avoid being socially chastised. They would rather take a jab that might maim or kill them than buck organizational systems or personal relationships.
II. The COVID Long-Hauler Syndrome is another coverup invented to conceal COVID vax injury.
The following is abridged from Pierre Kory’s Reports:
It took me a while to figure out why no patient in my hospital’s intensive care unit (ICU) ever had their vaccination status on the front screen of their record. It was instead stuck in the nursing notes where no one would look for it. And I learned that patients who had “unknown vax status” were being designated “unvaccinated.” Patients dying of Covid within two weeks of getting the shot were also called unvaccinated.
These methods persuaded doctors and nurses to believe that everyone in the hospital was unvaccinated. It also allowed our federal health agencies to create and disseminate charts showing that hospitals were filled with the unvaccinated. And they further manipulated even this false data.
These widespread frauds encouraged doctors to hector anyone and everything to get injected.
An ICU nurse sent me the following:
My friends on the night shift had stories to share about patients. All of them confirmed what we've seen - none of it makes sense unless you go to the 800 lb elephant in the room, the vaccine. We have not heard a peep from the vax cheerleaders on staff recently. I know some have buyer's remorse for pushing their family to get vaxxed, but there’s no need to dig into that wound now. Long Covid is the only term allowed, never vax injury.
Her last line really got to me. The standard practice is to blame all the strange illnesses on “Long hauler COVID” rather than “vaccination injury syndrome.” She continues:
Many employees as well as patients are participating in a Long Covid study - I know two employees in it. Don't know that it is providing them any answers to their disabling issues, especially at their young age, but they're hopeful. They are true believers - got fully vaxxed and boosted and will continue to do so. And they continue to contract Covid variants and pass them along to the rest of the same vaxxed-up cohort. Rinse and repeat. To bring up data that points to the exponential and cumulative harm is just pointless. They want to die on the hill of believing they did the right thing, no matter what their bodies are telling them. Until they can no longer do so.
I pulled aside an ED doc but we had to go outside to talk. And yes, our phones were off. In ED, patient issues are discussed in a kind of code if it concerns vax injury as the probable cause. Administrators wander through at all hours, so open discussions are not happening.
Residents are getting frustrated - I heard it’s coming out in staff meetings because they are seeing data and patients are bringing in data. Shift hand-off reports can get tense, I was told. Many are suffering from cognitive dissonance, "I have hundreds of thousands in med school loans. I cannot deviate or I lose everything and still have to pay back all that money. Must stick to what I am told." They become check-box doctors. You either sell your soul or seek your own data and then join the "French Medical Resistance.” This is not an easy call for a 20-something to make.
Not every patient is willing to walk in the dark about the severe issues they are having and believe the primary care physicians telling them there is nothing to worry about. The pushback from patients who decide to be informed is real, and the emergency docs have to find a way to address it before they admit or discharge a patient with some vague diagnosis. I see future liability expanding as the data keeps coming out. More patients are asking for their FULL medical record. They know. They know.
All the other stuff is still happening. We still have no space in the cancer hospital side for the explosion of pts needing treatment for their vax injuries - and it is NOT because they delayed cancer therapy due to the pandemic. It is NOT from delayed screening or treatment initiation. It's because they just received a new diagnosis that requires immediate intervention.
According to the same case manager I spoke with weeks ago who is carrying a patient load of almost 1000 now, she is trying to get creative and find space at outpatient facilities closed on weekends and schedule her teams and patients to go there. Those sites have full equipment, so they can give infusions at least. This is crazy. She called asking if we could open up space in another area - and yes, we are doing it.
Unsurprisingly, the diseases caused by the vax are still an unsolved mystery at Wikipedia: “While studies into various aspects of long COVID are underway, as of November 2021, the definition of the illness is still unclear, as is its mechanism.”
III. How To Treat the Vaccine Injured
Published June 18, 2022 on the Mercola blog. It was abridged and summarized by Yoho. This is the full PDF.
THE PANDEMIC OF VACCINE INJURIES
“My heart is so broken, I cannot keep quiet anymore,” Marik said, choking back tears during a Children's Health Defense hearing in Ohio where several vaccine-injured patients also shared their tragic journeys. "This is a humanitarian crisis! These people are suffering. This is real disease.”
Patients injured by the COVID jab say they receive little help when they go to the hospital. There are no specialized vaccine injury clinics. They have trouble getting care anywhere.
In the meantime, Pierre Kory’s Front Line Critical Care Alliance (FLCCC) is sharing their I-RECOVER protocol in the hope that doctors will begin to treat COVID jab injuries appropriately.
Dr. Kory states that COVID-19 is no longer an emergency. The true emergency is the continued use of the COVID vaccines, which are causing injuries on an alarming, unprecedented level.
He cites life insurance data showing historic rises in excess deaths for young people. The vaccine injuries reported to the U.S. Vaccine Adverse Event Reporting System (VAERS) are further support. Kory says that according to some estimates 500,000 Americans have lost their lives because of these shots. And the most highly vaccinated and boosted nations are experiencing record case and death rates from COVID compared to countries with lower injection rates.
THE POST-JAB AVALANCHE OF RARE DISEASES
Regardless of where the spike protein comes from — the shot, the virus, or close contact shedding — it produces many ill effects. The jab is the worst because it stimulates the body to produce still more toxic protein. Whether this ever stops is unknown, but early, aggressive, and appropriate treatment can help. This lowers the spike protein in the blood and reduces the risk of prolonged post-vax symptoms that the mainstream claims is long-haul COVID.
The jabs damage immune function, which is the first line of defense against all disease. Appendicitis and pediatric hepatitis have recently increased. Several rare forms of cancer have also become more common, and some of these are aggressive and fast-moving. In late 2021, pathologist Dr. Ryan Cole reported a 20-fold increase in endometrial cancer as well as a "massive uptick" in autoimmune diseases.
IVERMECTIN TREATMENT works well for the majority, while others benefit little. This drug has been used safely for over 50 years. A large-scale Brazilian trial studied people who received ivermectin for four days every month for six months. Not only were the chances of contracting COVID reduced dramatically, but kidney and liver function improved.
Dr. Kory says that published studies and experience with patients both prove that ivermectin is exceptionally safe. Marik adds, "It's one of the safest medications ... even when taken in high doses appropriately."
FLCCC VACCINE INJURY PROTOCOL: FIRST-LINE
The information below is a summary. Refer to this PDF link for the complete document.
Ivermectin — 0.2 to 0.3 mg/kg, daily for up to 4 to 6 weeks. It is taken with or just following a meal for best absorption. Some people respond to it and some do not. Ivermectin has potent anti-inflammatory properties and binds to the spike protein, which improves its elimination.
Vitamin C — 1000 mg orally three to four times a day. Note: these high doses are not recommended for indefinite daily use. C helps promote the growth of protective gut bacteria. Avoid high dose C in patients with a history of kidney stones.
Vitamin D — reasonable starting doses are 4,000 to 5,000 IU (international units) per day. This should be adjusted by measuring blood levels. (Yoho note: Vitamin D levels for Florida lifeguards can be 120 ng/ml. Getting your levels over 60 ng/ml—or better, near 100 ng/ml—is thought by many authorities to be advantageous. You may need more D than Dr. Mercola advises to accomplish this. Doses are individual.)
Vitamin K — 100 mcg/day.
Quercetin — 250 to 500 mg/day (Mixed flavonoids are an alternative). These are anti-inflammatory. Due to a possible drug interaction between quercetin and ivermectin, these drugs should not be taken at the same meal. In rare cases, quercetin has been associated with hypothyroidism, so it should be used with caution in patients with this problem. Physicians should consider checking thyroid hormone blood levels.
Magnesium — 500 mg/day.
FLCCC VACCINE INJURY PROTOCOL: SECOND-LINE
Hydroxychloroquine (HCQ) 200 mg twice daily for 1–2 weeks, then reduced to 200 mg/day. This is safe in pregnancy. For long-term use, and for patients weighing less than 135 pounds, the dose should be reduced to possibly 100 to 150 mg/day.
Intravenous vitamin C — 25 grams once a week. The first weekly IV dose should be lower, 7.5–15 grams. Vitamin C is given slowly IV over 2–4 hours, together with the oral form, 1000 mg 2–3 times per day. Since vitamin C can cause kidney stones, the length of therapy must be limited.
N-acetyl cysteine (NAC) — 600–1500 mg/day.
Low dose corticosteroid — 10–15 mg/day of prednisone or the equivalent for three weeks. Taper to 10 mg/day and then 5 mg/day as it is discontinued.
For the complete list, see the I-RECOVER Post-Vaccine Treatment Protocol, which is available on covid19criticalcare.com.
Yoho note: This protocol is predictable and safe, but some of the recommendations from the full list are speculative. You need supervision by a licensed physician.
I won’t waste your time quoting Wikipedia about Ivermectin “disinformation.”
IV. How to order ivermectin and other drugs abroad
First, read what Butchered by “Healthcare” says about mail ordering drugs:
Since patented medications are more dependable than generics, look for them overseas. Most manufacturers sell their patented drugs in other countries at a fraction of the US price, often using another brand name. You can purchase them by mail-order from foreign pharmacies’ websites. Some are over-the-counter there, making this easy.
Some drugs are 50 to even 98 percent less costly than in the US. For example, in late 2017, the brand name Viagra was $65 here for a single 100 mg tablet and $30 for the authorized generic. By early 2020, GoodRx.com, which compares US-based pharmacies, was offering this generic for around $12. Check for updates on their website. But various Indian websites sell the same medication for $1. I have a close friend who tried the Indian version and he said it was a little weak but worked fine.
The drug industry calls this reimportation, and they aggressively oppose it, supposedly to protect quality. Several state governments have championed their citizens’ rights to order abroad, however. There were congressional fights in the early 2000s to make this lawful nationwide, but our bought-and-paid-for legislature continues to block it. The compromise seems to be to leave it illegal but not prosecute anyone.
Since the FDA does not reach out of the US, there are more quality issues abroad. A maker might fake a brand name. A generic might have no active ingredients or even contain contaminants. But by 2014, wholesalers were importing 80 percent of the drugs and ingredients used here, anyway. European pharmacies get most of their drugs from other countries as well.
PharmacyChecker.com can tell you if the medications ordered overseas are likely OK. The best policy is always caveat emptor. Learn as much as you can before you buy and observe the effects of anything you take. And be just as careful at Walgreens as when buying internationally.
The following is a pharmacy in India that sells many drugs including ivermectin. I have heard good things about them, but there are never guarantees about the legality of ordering medicines overseas nor about their quality. And there are many other pharmacies.
SUNRISE ENTERPRISE
export@sunriseindia.org
A-206, 2nd Floor, Sumel Business Park-6
Dudheshwar Road
Opposite Hanumanpura BRTS, Shaibaug
Ahmedabad, State-Gujarat (India)
Whatsapp - +919099096658







Share this post