


READER RESOURCES: THE APOCALYPSE ALMANAC: Hidden cures in our dystopian age. Check out the “Cure Cancer in Your Kitchen” chapter. FULLSCRIPT SUPPLEMENTS: top quality and economical. AFFILIATE STORE: I offer competitively priced products HEREthat I have personally tested and used.
Summary
• Two operations reduce a large breast. One involves cutting and sewing for hours under general anesthesia and has published complication rates of 40 to 50 percent. The other uses three or four pinhole incisions, takes less than an hour, and can be performed under local anesthesia if the technique is appropriate.
• The cut-and-sew operation severs the blood supply and nerves, ends breastfeeding, decreases nipple sensation in many women, and, on occasion, destroys the nipple itself through tissue death.
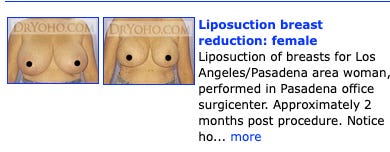
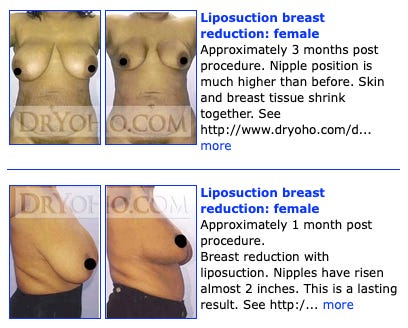
• Liposuction reduction lifts the nipple by up to 3 inches, preserves milk ducts and sensation, leaves almost no scar, and, in trained hands, has near-zero complication rates.
• A landmark 1993 paper and a 2024 systematic review both support liposuction for reduction in appropriately selected patients. Plastic surgeons have ignored 30 years of evidence.
• Insurers pay the plastic surgeon roughly 10,000 dollars and the surgical facility tens of thousands for the bloody operation. They classify the gentle one as cosmetic and unproven, and pay nothing.
• The money determines which operation a woman is offered. The clinical evidence points the other way.

The operation nobody offers
A woman with heavy breasts walks into a plastic surgeon’s office, complaining of back pain, with deep grooves carved into her shoulders by bra straps, and a wish to stand straight again. She is offered one operation. The surgeon draws a keyhole pattern on the skin, lifts the nipple on a stalk of tissue, and cuts out pounds of breast tissue. Then he sews the whole thing together, leaving a scar around the areola, a scar running down the front, and often, a scar in the crease underneath.
The operation takes hours. She goes under general anesthesia. She may wake with no feeling in her nipples and will have no ability to nurse. She is told this is the price of relief and that this trade-off is normal.
She is almost never told that a second option exists. That operation removes the same amount of weight in three or four cuts, each no wider than a pencil. It can be performed under local anesthesia or light sedation, takes well under an hour, and leaves sensation and milk ducts intact, with no scar worth mentioning.
The reason she never hears about it is money. The bloody operation often pays the surgeon and the facility tens of thousands of dollars. The gentle one pays cash, and not much of it. That single fact has shaped what two generations of women were allowed to know about their breast surgery options.
A method with 30 years of evidence behind it
Liposuction breast reduction is neither fringe nor new. The thread goes back four decades in the surgical journals, and every step points in the same direction.
In 1985, Bahman Teimourian introduced liposuction of the breast as an adjunct to reduction. In 1991, Alan Matarasso and Eugene Courtiss reported using suction alone to reduce large breasts in their paper “Suction Mammaplasty: The Use of Suction Lipectomy to Reduce Large Breasts”. They limited the method to women with well-placed nipples and fatty breasts. Two years later, Courtiss removed even that restriction.
His 1993 paper, “Reduction Mammaplasty by Suction Alone,” in Plastic and Reconstructive Surgery reported that longstanding concerns about nipple size, nipple position, and the cause of enlargement were unfounded. His patients ended up with pleasing breasts, good sensation, and minimal scars. He concluded that suction alone is the technique of choice for selected women.
Lou Gray updated the record in 2001, reporting 204 women. Lloyd Habbema published a large series in Dermatologic Surgery in 2009, using tumescent local anesthesia and powered cannulas. A 2024 systematic review in Aesthetic Plastic Surgery pooled modern outcome data and concluded that liposuction-only reduction is safe and effective, improving patient satisfaction, reducing volume, and correcting sagging, with far fewer complications than the cut-and-sew approach.
Thirty years of evidence sit in the journals. The profession that publishes those journals has spent those same 30 years steering patients away from what the evidence shows.
How a large breast comes out through a cannula
The objection sounds reasonable at first. A breast is a gland, the thinking goes, so a fat-removal tool cannot reduce it. But this objection collapses under anatomical scrutiny.
A mature breast is mostly fat. Breast composition shifts with age from dense glandular tissue toward fatty replacement, and in most adult women the fat fraction is high. One breast computed tomography study found that even dense breasts seldom exceeded 50 percent glandular tissue and that most women are better described as 70 percent fat. In heavy, sagging breasts outside of pregnancy and nursing, the fatty share climbs higher, toward 90 percent in many cases.
Fat is soft and passes easily through a cannula. Glandular tissue is firm and resists suction. The high fat content of the large adult breast is exactly what makes it a liposuction target. The cannula removes the soft bulk that contributes to weight while leaving the firm glandular core, ducts, and vessels intact.
Exceptions exist. Young women with dense, firm breasts have a lower fat fraction, so a cannula does less for them. A breast that is mostly skin and a stretched envelope rather than volume needs a lift, not a reduction. A careful evaluation sorts these cases out before surgery. For the large, fatty breast that accounts for the vast majority of reduction requests, the cannula is the right tool.
What the cut-and-sew operation does to a breast
Standard reduction is a three-dimensional puzzle. The surgeon must lift the nipple into a youthful position, remove large amounts of tissue, and attempt to preserve the blood supply to the breast skin. To raise the nipple, he cuts half of the skin attachments around the areola, the pigmented area surrounding the nipple. The procedure partially destroys the circulation and nerve supply.
For large breasts, he uses electrocautery to cut through tissue and control bleeding. Blood that collects under the sewn-up reconstruction presses on the remaining tissue, potentially cutting off its blood supply. The outcome is not fully predictable even in expert hands, because the surgeon is gambling on whether the tissue stalk he has left to support the breast will supply enough blood.
When the gamble fails, the nipple-areolar complex, the pigmented area, dies in part or in whole. Reported rates of nipple-areolar tissue necrosis range from roughly 2 percent to 13 percent, depending on the technique, with the superior and medial pedicle methods at the higher end. This describes the anatomical location where the surgeon preserves the blood supply. A 2025 meta-analysis of more than 71,000 patients found that complications after reduction mammaplasty occur at rates as high as 40 to 50 percent: bleeding, wound breakdown, nipple necrosis, infection, fat necrosis, asymmetry, and loss of nipple sensation. Surgeons with massive experience who are true artists achieve far better complication rates, but they remain significant.
Obesity worsens outcomes. A study of complications by body mass index found a clear pattern among patients who developed them. Every case of nipple necrosis and nearly every case of fat necrosis occurred in women with a body mass index of 30 or higher. This is classified as obese, with 32-40% body fat. The heavier the woman, the more tissue the surgeon must move, and the more the blood supply is pushed to its limit.
Even when the result looks good, the woman may have little or no sensation in her nipples. Some of the nerves were cut to reposition the nipple, and that sensation may not return. For some women, the loss is permanent and total, and no one warned them that this was a common outcome rather than a rare mishap.
Hours under general anesthesia, and the risk that comes with it
The cut-and-sew reduction takes hours, sometimes five or more. It is performed under general anesthesia, which carries a risk of death independent of the surgeon’s actions. The longer the operation, the greater the exposure to blood loss, clots, and the cardiac strain from prolonged sedation.
Complications rise when surgeons combine procedures. Fatalities occur, especially when an aggressive breast operation is paired with another lengthy procedure, such as a tummy tuck, in the same session. (Tummy tucks create scars that can be two feet long and carry a high complication rate and a significant death rate.) The combined operating time, blood loss, and anesthetic load multiply the danger. The marketing calls it a mommy makeover. The death certificates call it something else.
Comment: I competed against plastic surgeons for 30 years. I watched them push the long operation because it paid, and disparage the short one because it did not. Their philosophy was almost purely financial, to a man.
Half an hour, three small cuts, no scar
Breast reduction by liposuction is routine for a surgeon with high-volume body liposuction experience. Even for large breasts, it takes 15 to 45 minutes in experienced hands. The incisions are three or four 3- to 4-millimeter cuts, wide enough to admit the cannula and anesthetic and nothing more. Complications are close to unheard of, though in this work no one ever says never, and even cosmetic surgery fatalities happen at least once in a career to almost every surgeon.
The skin shrinks and the nipples elevate as healing occurs. Published series report a lift of roughly 2.5 centimeters (an inch). In a liposuction breast reduction study, older patients experienced lifts exceeding 3 centimeters. The study reported a 93 percent satisfaction rate and volume reductions of nearly 700 milliliters per breast. The lift is the surgeon’s primary goal in reconstruction and was achieved here without a single noticeable incision or nerve cutting.
Comment: Throughout my career, I performed about 10,000 liposuction procedures, including many large-volume cases up to 10 liters. Breast liposuction is straightforward, and with this background, I knew how to be aggressive. Breast circulation is excellent if you don’t cut the structures you would in a breast lift, and I never had any skin necrosis or significant problems.
As the breast heals, it softens into a smooth, pleasing shape. The cosmetic result rivals that of an average cut-and-sew reduction. The nipple retains its blood supply because nothing was detached, and it retains its sensation because nothing was cut. If the contour does not satisfy the patient once the swelling has settled, a lift can be performed six months later. This carries far less risk and far less damage to the milk ducts than a primary reduction.
The technique that separates a good result from nothing
What makes this work is the tumescent method, developed by the dermatologist Jeffrey Klein. The surgeon floods the breast with a large volume, often many liters, of dilute local anesthetic mixed with adrenaline. The fluid swells the tissue, making it firm (tumescent). Dr. Klein said he chose the word because it sounded sexy and safe. The adrenaline clamps the small blood vessels shut, which all but eliminates bleeding and bruising.
The safety record of tumescent anesthesia is the strongest argument against the general-anesthesia model. The diluted solution, infused via a power pump and small cannula, allows the surgeon to use far more lidocaine than the old textbook limit without toxicity, because the drug is absorbed slowly over many hours and much of it is suctioned out with the fat. A study in Dermatologic Surgery found doses up to 55 milligrams per kilogram to be safe for liposuction, compared with a conventional infiltration limit of 7. Other literature suggests that even higher doses can be used. The Indian standard guidelines of care for tumescent liposuction note that hundreds of thousands of cases have been performed with no reported deaths when tumescent anesthesia is used alone.
Sedation can be added for comfort. The patient remains awake, breathing on her own, and avoids the hazards of general anesthesia. The contrast is stark. One method uses a drug delivery so safe it has no recorded body count when used alone. The other puts the patient fully under for hours and accepts a significant, well-known mortality risk as the cost of doing business.
Comment: The anesthesiologists deny that general anesthesia carries a significant fatality risk and even cite literature supposedly confirming this. Who would believe them? They are in the business, and their policy is to always point the finger at the surgeon. I wrote about all this in my peer-reviewed paper, which is cited in the references, so I am an expert. For years, I used a propofol and ketamine technique for sedation, but I dropped the ketamine after a while. I developed a way to dilute propofol. With properly applied and adequately dosed tumescent local anesthesia, the ketamine added risk and gave me nothing.
Skill is the critical variable. The surgeon must be aggressive enough to remove significant volume. A timid operator removes too little, and nothing happens: no lift, no change in size. The work requires the mindset of someone who has performed thousands of liposuction cases, not a few per year.
Here is a way to understand risk numbers.
A surgeon with a long career sees a 1-in-4,000 risk arrive in person. It happens. It is rare, and he has seen it. A 1-in-100,000 risk is one he likely never encounters. The gap between those two numbers is the whole argument, because the two operations sit on opposite sides of it.
The anesthesiologists’ favorite number is a ridiculous fiction. They cite an anesthesia death rate near 1 in 300,000, but a review I published of the surgical risk literature found that figure was extrapolated, not measured. The landmark Lagasse analysis, cited at the end of this article in my reference about cosmetic surgery mortality, surveyed the entire published literature in 2002. It estimated true anesthesia mortality near 1 in 13,000. That is not a number a surgeon meets once in a lifetime. It is a number he will have or has had experience with.
General anesthesia is the thread tying together the worst outcomes. Plastic surgeons, who favor it, have reported liposuction death rates near 1 in 5,000. Dermatologists, who use tumescent local anesthesia and almost no general anesthesia, reported zero deaths in 66,570 liposuction cases in a national survey. Same operation, different anesthesia, and the body count shifts from steady to none.
The danger multiplies when operations are combined. The same surgical literature shows liposuction death rates rising roughly 14-fold when the procedure is added to a tummy tuck. The lesson points in one direction: shorter surgery, lighter anesthesia, one procedure at a time. The buried operation is all three. The bloody one is none of them.
Breastfeeding survives one operation and not the other
After a cut-and-sew reduction, nursing is typically impossible. The operation removes glandular tissue and severs the duct and vessel network that produces and delivers milk. A young woman who undergoes this type of breast reduction before having children later finds she cannot breastfeed, and no one had made that consequence clear to her beforehand.
After liposuction, breastfeeding is almost never affected because no ductal tissue is removed. The cannula removes fat while leaving the milk-producing tissue intact. A woman has her breasts reduced at 25 and nurses a baby at 30, with the ducts intact. We have seen this many times in practice. For a woman who wants both relief and the option to nurse later, the choice between the two operations is clear.
Aftercare
A supportive molding bra is critical during recovery and should be worn day and night for the first weeks to maintain the new shape while the skin and other breast structures contract. Breast massage during the postoperative period helps reduce firmness and angularity, which resolve more quickly by breaking up the temporary hardness that follows liposuction.
Most patients return to normal activity within 24 to 48 hours, not weeks, because there is no large wound to heal and no tissue stalk whose survival the surgeon must monitor. Within a few months, the final contour emerges, often as pleasing as that of a breast lift that costs many times more but without the scars. Significant complications are vanishingly rare, and skin loss almost never occurs because the blood supply is never severed.
Follow the money
Here is why a woman is steered toward the bloody operation. Insurance reimburses the cut-and-sew reduction handsomely. The plastic surgeon collects about $10,000 for the procedure. Whoever owns the surgical center, often the operating surgeon himself, may collect another $40,000 to $50,000 from the insurer for facility charges. The plastic surgery profession spent decades maneuvering insurers into paying for all this.
The insurers built the bias into their coverage rules. The cut-and-sew operation has billing code 19318, and insurers pay for it as medically necessary once a woman meets the weight thresholds. Liposuction-only reduction has a different code, 15877. One major insurer’s breast reduction coverage policy classifies liposuction-only reduction as unproven, not medically necessary as a sole treatment for large breasts, and not separately reimbursable. The gentle operation is removed from the menu before the patient even walks in.
Liposuction reduction is a cash market for that reason. Insurance does not cover it. Surgery centers do not reimburse for it because it is classified as elective and cosmetic. No insurance check means no doctor enthusiasm. So plastic surgeons rarely learn the technique and disparage it to patients with a parade of oddball objections about contour, recurrence, and missed cancers, none of which holds up under scrutiny of the outcome data.
The cancer worry, in particular, is weak. The cut-and-sew operation scars the breast tissue and distorts the architecture a radiologist reads on a mammogram, whereas liposuction leaves it largely intact. In a case I published with a colleague, a woman’s mammogram 11 months after breast liposuction showed only a smaller breast and no postsurgical changes.
A second force keeps the technique buried. Plastic surgeons hold a near-monopoly on reconstruction skills, so insurers pay them handsomely for it. Breast liposuction skills are easier to acquire but less well known within the surgical mainstream, and because it pays in cash only, “real surgeons” rarely bother to master it. Surgeons from other specialties who do perform liposuction often lack the surgical training and the aggressive hand large breasts demand. Plastic surgeons, for their part, generally never learn tumescent anesthesia or high-volume body liposuction at all, and default to general anesthesia. They do without the “tumescent” anesthetic-adrenaline mix that controls pain and bleeding and protects the tissue against the trauma of the procedure.
Comment: The math is not subtle. One operation pays the surgeon and the facility tens of thousands of dollars, while the other is cash-pay and takes 40 minutes. Guess which one gets recommended in the consultation room.
Building the case for the insurer
Reimbursement does not arrive unbidden. The surgeon must prove medical necessity, and the threshold is a weight of tissue tied to the patient’s body size. Most insurers use a sliding scale that requires a minimum number of grams removed from each breast. Clear the bar, and the claim is paid. Miss it, and the operation is cosmetic, and the surgeon collects nothing.
A board-certified plastic surgeon writing for patients states that he regularly receives requests to lie for insurance approval. He warns that a surgeon willing to do so commits insurance fraud. He adds that the weight scale insurers rely on is used against the wishes of the researcher who created it and against a standing statement from the American Society of Plastic Surgeons.
The incentive to manufacture necessity is built into the system and acknowledged within the profession. The medical record is dressed to fit the threshold. Symptoms are inflated. Physical findings are invented or exaggerated.
Photographs are angled, lit, and selected to make breasts look larger and the shoulder grooving from the weight of the bra, which supports the breasts, deeper than the exam supports. Imaging is ordered and read to document a problem that justifies the knife. The paperwork is built backward from the reimbursement code, not forward from the patient.
Comment: I have reviewed these charts. I found records documenting outright lies to insurers, fabricated physical exams, and imaging dressed up to justify the fee. Sometimes other patients’ photographs are used and submitted to the insurer. Patients rarely complain because they are getting surgery that is discounted or free, and the surgeon and the surgery center are splitting tens of thousands of dollars of someone else’s money. Everyone in the room is happy except the insurer (and what do they care? They raise the rates). In the end, we all pay higher premiums to cover the cost of the theft.
None of this is necessary for gentle operation because no insurer is paying for it. The cash patient needs no manufactured necessity, no inflated grams, no staged photograph. She wants smaller breasts and pays for them. The fraud lives entirely in the insurance payment that makes the big bucks for those who game the system, and this is nearly everyone involved in getting paid.
What the official sources tell her
A woman who tries to research her options finds the same bias repeated everywhere she looks. Wikipedia entries, hospital pages, and surgical society materials all present the cut-and-sew operation as the standard. They treat liposuction as a minor footnote for a narrow slice of patients, if they mention it at all. It reads like settled medical consensus. It is the marketing of a profession that profits from insurance reimbursement and sometimes from fraud.
The pattern repeats across every corner of medicine, where a cheaper, gentler, and safer treatment threatens a lucrative one. The institutions that write the official version are funded by, staffed by, and built around the people who bill for the expensive procedure. Their account of the evidence is the house position of an industry, dressed up as an objective fact.
The caveat
The technique fails in unskilled hands. Inexperienced liposuction surgeons do not understand breast work and are generally not aggressive enough. Remove too little fat, and the breast does not lift or shrink. The procedure is simple in principle but unforgiving of timidity.
Comment: I saw areas of skin death in a small percentage of my large-volume liposuction patients and larger areas in a rare few; however, I never saw anything like this in breast liposuction.
This procedure is not for every breast. The young woman with dense, glandular tissue and the woman whose problem is a stretched skin envelope rather than volume both need something else. A surgeon who promises a cannula will fix every breast is as dishonest as one who pretends it fixes none. The truth lies somewhere in between, and it has nothing to do with the oddball dangers the plastic surgery profession claims befall its competitors’ patients.
Comment: The competition was not friendly. The plastic surgeons reported to the Medical Board anyone they disliked and badmouthed us to patients. When they could not cast aspersions on results, they attacked credentials and paperwork. That is what a guild does when a better, cheaper method threatens the franchise.
No surgeon can claim a zero-complication rate, and anyone can be criticized for a serious complication. It’s a fractious, litigious, adversarial environment for all cosmetic surgeons.
Critical Counterpoint
There are cases where traditional breast reductions with the anchor scar are the only good option, and in skilled hands, the complication rate probably falls below 5%. The problem is that few breast reduction surgeons know anything about liposuction surgery and aren’t interested in it because it’s not financially remunerative. This keeps them from properly comparing these options for their patients when they come to consult. I have watched many breast reduction surgeries, and they are sometimes butcher jobs.
The safest and most accurate option for large, mature breasts is to do breast liposuction first, wait four to six months, and then do the breast lift. This isn’t instant gratification, but I want you to read that sentence over again if you are thinking seriously about breast reduction. You don’t have to use the same surgeon for the two procedures. In fact, few breast lift surgeons are qualified to perform liposuction. They would say, with accuracy, that the reverse was also true.
However, I have one colleague who is a true artist at this surgery, and he can do something that’s almost more difficult, which is to remove the material around an encapsulated implant, both scar and extruded silicone in one piece, to treat breast implant illness. This is at least a 4-hour procedure and requires patience, a strong back, and deft technique.
So I’m going to do something here that I don’t usually do: recommend a doctor. His name is John Walker, MD, and I don’t have any financial relationship with him. I would not make a recommendation like this except that trustworthy and highly skilled breast surgeons are hard to find. His expertise is uncommon and not easily acquired. Dr. Walker has done several thousand of these procedures, including for my wife and my daughter, where he removed the implants and took out all the material around them and didn’t do the lift. Although this surgery is never cheap, he is reasonably priced for what he does.


Results like the above take a lifetime of practice to attain.
I have many photographs of Dr. Walker’s work behind the paywall, so if you are considering him, please subscribe to view them.
Again, if you think you are sick because of your breast implants, you may have breast implant illness (BII). In this case, you need your implant removed along with the surrounding material in one piece. Once again, this is a painstaking operation that requires great experience and patience.



Dr. Walker’s office cell phone number is +1 (424) 448- 9189, and his website is https://bpspinc.com. You can text to get in touch.
If seeing Dr. Walker is not convenient, you should consider seeing Dr. Khan, who specializes exclusively in this procedure, has cured thousands of women, and has dozens, if not hundreds, of testimonials on his website. I wrote a comprehensive article about breast implant illness and his practice HERE that includes his contact information. His rates are not exorbitant, and he is also highly skilled.
I don’t believe Dr. Khan performs breast lifts. His work focuses on treating BII by completely removing implants and the infected, contaminated tissue and foreign substances around them. Here is a patient testimonial, and it is typical for this physician:
I just explanted with Dr Khan a little over two weeks ago. Dr Khan is everything they say he is; what all medical professionals should be. You will get the best care and peace of mind that everything was removed so you can begin to heal. A few months ago I thought I was dying. I, too, had all but 5 symptoms. The day after surgery I felt life return to me. I had more energy than I’ve had in years. I was up and walking. I could breathe deep breaths without pain. The gritty sandpaper eyes no more. It was simply amazing! Every day I get better and better. You will be here too. I traveled from CA to MI. The best decision I could have made.
Although I know Dr. Walker far better than Dr. Khan, I recommend both surgeons without qualification. It is worth taking a plane trip to see either of these people.
I have a postscript, and that is that although saline implants can get hard and cause breast implant illness and other problems, this is far more likely with silicone-filled implants. After meeting Dr. Khan, I believe that silicone-filled implants are unethical and should be banned. Even saline implants are questionable because they, too, can cause health issues and sometimes major medical problems.
PPS: Shopping for a liposuction surgeon is easier, but you must respect experience. You want someone who has, ideally, performed large-volume liposuction of 8 L or more and is confident with breast liposuction. Surgeons like this usually won’t be intimidated by the prospect of breast liposuction. They should be able to quantify the volume they can take off your breasts. If you’re an older woman, since your breasts are statistically mostly fat, this is relatively predictable in experienced hands.
Closing
A woman with heavy breasts deserves to hear about both operations before she chooses. The one she is typically offered pays the people offering it and requires her to accept permanent nerve damage, loss of sensation, damaged milk ducts, three long scars, hours under anesthesia, and a significant risk of losing a nipple. The one she is not offered would leave her with sensation, the ability to nurse, nearly invisible scars, and an hour of recovery instead of a season. Cosmetic results in properly selected patients are somewhat different, but given the trade-offs, are often equivalent.
Thirty years of surgical literature say the buried operation works for the patient it suits. The silence around it is not a medical judgment. It is a financial one, encoded in the billing system and repeated until it sounds like science. A woman who learns the difference knows to ask for the operation nobody offered her. Most never get the chance.
Selected references
I authored the last four, and Reference 12 was my major paper in a peer-reviewed journal. Thirteen was about my superior anesthetic technique.
1. Reduction mammaplasty by suction alone (Courtiss, Plastic and Reconstructive Surgery, 1993)
3. Liposuction-Only Breast Reduction: A Systematic Review of Outcomes (Kadhum et al., 2024)
5. Breast reduction performed by liposuction (Journal of Cosmetic Dermatology)
7. Postoperative Complications Following Reduction Mammaplasty in Relation to Patient Body Mass Index
9. Tumescent liposuction: standard guidelines of care
10. Reduction mammaplasty coverage policy classifying liposuction-only reduction as unproven
15. Liposuction in Breast Reduction: the “No Scalpel Breast Reduction” (archived)
Note that the last four references are archived in the Wayback Machine. If you are interested, click on some of the links in these references. If you do, you will see the 2000-page website that I had up for 30 years to show my patients and potential patients what I did. It was DrYoho.com, but now I have a backup at that site.
But wait, there is more!
Behind the paywall below, I have a follow-up on my experience and my readers’ experience with thiamine therapy for neurological diseases.
Breast lift before-and-after photos by Dr. Walker. Note: these are graphic, and if you are disturbed by that, don’t look.
My academic article on how breast liposuction does not alter mammogram results.
And I copied the best article I’ve ever read on choosing your cosmetic surgeon.
Listen to this episode with a 7-day free trial
Subscribe to Surviving Healthcare to listen to this post and get 7 days of free access to the full post archives.




